2018 ADA Summary of revision
General changes
- 從2018起,如果出現新的證據,ADA會更常線上更新治療準則。
- Standards of care現在是ADA 唯一臨床建議指引。
- 有些建議的證據等級有改變,這些改變沒有標示在summary of revision中。
Section changes
Section 1. Improving care and promoting
health in population
- 整個section的名字改了。
- 增加了使用可信賴的資料指標來評估併改善糖尿病照護品質和減少支出。
- 增加關於族群健康在社會面向的討論。
- 增加關於在糖尿病照護中使用遠距醫療的討論。
Section 2. Classification and Diagnosis
of Diabetes
- 加入建議:要釐清使用HbA1C的時機和限制:
- 例如有紅血球變異、實驗方法干擾、或是會影響紅血球的turnover的狀況
- Sick cell disease、懷孕第2第3孕期的孕婦、洗腎病人、 最近有失血或輸血的病人、 使用EPO的病人,要用plasma
glucose criteria 來診斷DM (而非A1C)。
- 針對小孩和青少年族群篩檢糖尿病前期和第2型糖尿病的建議改變了
- 改成有過重或肥胖加上1項以上的危險因子就要去篩檢
- (表2.5) 過重(BMI> 同年齡性別的 85百分位、BW or BH > 85百分位、或BW>120% 理想體重),加上以下1項以上的危險因子:
- 母親有糖尿病或懷該小孩時有妊娠糖尿病
- 1等親或2等親有T2DM
- 某些種族(Native
American, African American, Latino, Asian American, Pacific Islander)
- 胰島素阻抗的表現或相關表現: 黑色棘皮症、高血壓、高血脂、PCOS、small for gestational age birthweight )
- 雖然一般不被建議,在有陽性結果時可以有足夠轉介資源的地方可以考慮做社區篩檢。
- 加入討論器官移植後糖尿病病人的細節。
Section 3. Comprehensive Medical
Evaluation and Assessment of Comorbidities
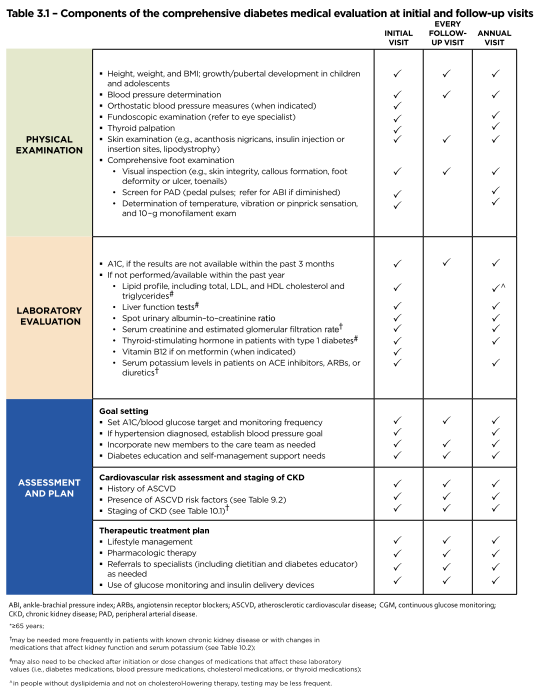
- Table 3.1重新整理 告訴我們在第1次看到病人和之後追蹤要做哪些評估
- Table 3.1

- 疫苗章節配合CDC建議做修正。
- 加入在以病人為中心的照護要注意選擇病人語言的敘述。
- 胰臟炎被加入共病症的部分
- 包括新建議: 考慮在需要接受全胰臟切除的慢性胰臟炎病人,作自體胰島移植來預防手術後的糖尿病。
- 加入考慮在有hypogonadism表現的糖尿病男性病人,抽血液testosterone level。
Section 4. Lifestyle management
- 一個建議被修正:有效率的糖尿病自我照護教育和支持應以病人為中心,可以從個人、團體或是科技平台著手,而且應該要對做出臨床決策有幫助。
- 釐清ADA對飲食的建議:對於巨量營養素沒有單一理想的比例,飲食計畫應該要個別化 (individualized)。
- 文字加上對低碳水化合物飲食的描述
- " 低碳水化合物飲食對糖尿病病人的腳色仍不清楚,一部分是因為 "低碳水化合物"
的定義各家不同,範圍很廣,雖然有些好處被描述,這些幫助傾向是短期的,並且隨著時間變化,這些效果並不會長期維持。 "
- "有些研究顯示極低碳水化合物飲食(verylow–carbohydrate) 或生酮飲食
(ketogenic diets) (一天小於 50-g CHO) 可能會帶來好處,如果病人想嘗試,這些方式只適合短期 (到3-4個月)。因為並沒有研究來證明長期這樣飲食是否會帶來好處或是傷害。" (S43)
Section 5. Prevention or Delay of Type 2
Diabetes
- 根據DPP研究結果,調整了對於用metformin來預防pre-DM的文字敘述。
Section 6. Glycemic targets
- 對T1DM使用CGM 的建議,不再侷限25歲以上,而推廣到所有成年(18歲以上) 血糖沒有達標的病人。
- 介紹最近被核可在成年人使用的,新的intermittent or “
flash” CGM device。
- The intermittent or
“flash” CGM device, very recently approved for adult use only (18),
differs from previous CGM devices. Specifically,it does not have alarms,
does not require calibration with SMBG, and does not communicate
continuously (only on demand). It is reported to have a lower cost than
traditional systems. A study in adults with well-controlled type 1
diabetes found that flash CGM users spent less time in hypoglycemia than
those using SMBG (19). However, due to significant differences between
flashCGM and other CGM devices, more discussion is needed on outcomes and
regarding specific recommendations. (S56)
- 加入了用 “不需要用SMBG校正的新的 CGM 裝置” 來調整治療決策的細節
- For most CGM systems,
confirmatory SMBG is required to make treatment decisions, though a
randomized controlled trial of 226 adults suggested that an enhanced CGM
device could be used safely and effectively without regular confirmatory
SMBG in patients with well-controlled type 1 diabetes at low risk of
severe hypoglycemia(1). Two CGM devices are now approved by the U.S. Food
and Drug Administration (FDA) for making treatment decisions without SMBG
confirmation (18,20), including the flash CGM device. (S56)
- 一樣強調A1C的限制。
- 把level 1 hypoglycemia從原來的” glucose alert value” 重新命名為”
hypoglycemia alert value”。
Sect 7. Obesity management for the
treatment of Type 2 Diabetes
- Table 7.2 加入了國家平均取得之藥價(NADAC price)。
Section 8. Pharmacologic approaches to
glycemic treatment
- 加入新的建議:建議有ASCVD的病人,治療的選擇,要從生活型態改變和metformin開始,之後配合可以減少心血管疾病事件和心血管疾病造成的死亡的藥物 (目前是empagliflozin 和liragluide (建議等級A),canagliflozin (建議等級C)) 。
- 加入了新的Table
8.1。Fig 8.1 和 Table 8.1可用來幫助選擇治療藥物以及幫忙做SDM (共享治療決策)。
-
- Table 8.2 修正來強調美國境內可用的降血糖藥物藥理學和機轉



- Table 8.3, 8.4 加入藥價資訊

Section 9. Cardiovascular Disease and
Risk management
- 加入新建議:建議所有高血壓的糖尿病病人應該在家量血壓,來幫忙確認masked hypertension or
white coat hypertension, 也可以改善服藥行為。
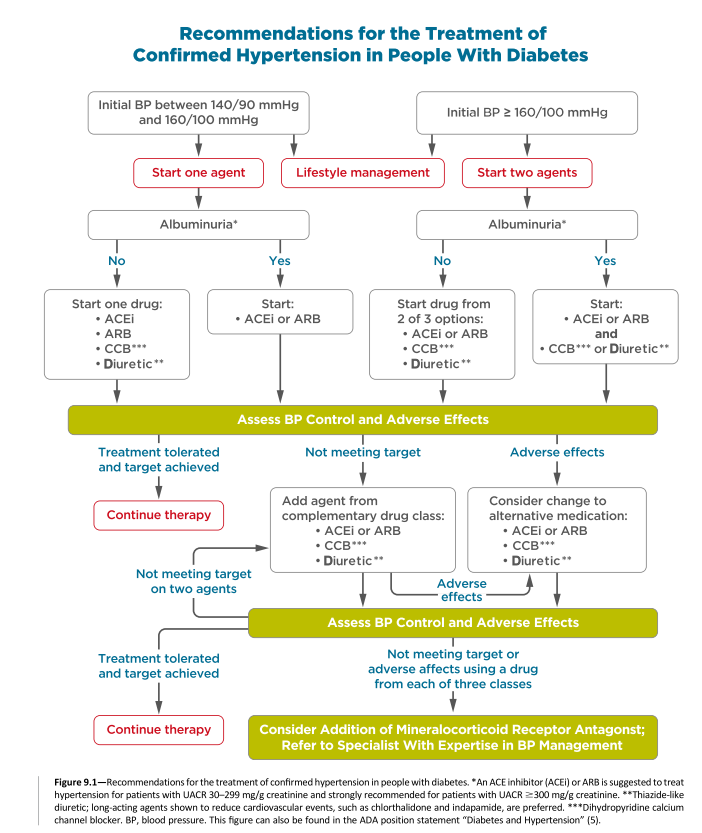
- 加入新的Fig 9.1 來建議同時有糖尿病和高血壓的病人如何選擇藥物。
- 加入新的Table 9.1 來比較比較積極和標準血壓控制的各項研究

- 加入新建議:建議在難以治療的高血壓病人考慮使用mineralocorticoid receptor antagonist。
- 血脂建議修正為強調風險:根據風險分為2群:有ASCVD 和沒有的
- 因為研究結果在老人和中年人好處類似, 40-75歲和> 75歲沒有ASCVD的病人建議使用moderate
intensity statin
- Table 9.2 也據此更新了
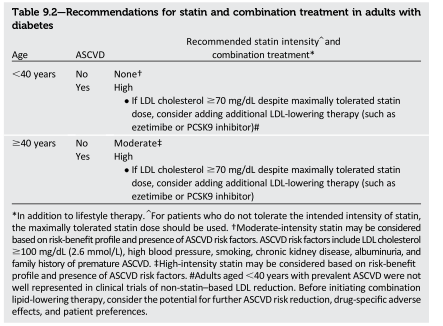
- 加上使用非statin 降LDL藥物的建議:
- 同時有糖尿病和ASCVD的病人,如果使用最大容忍劑量的statin,LDL 還是>=70mg/dl, 考慮使用額外的降LDL藥物 (如ezetimibe 或PCSK9 inhibitor)。 在評估CV 風險,藥物副作用和病人選擇後,Ezetimibe可能是較優先的選擇, 因為藥價較低 (建議等級A)
(S92)
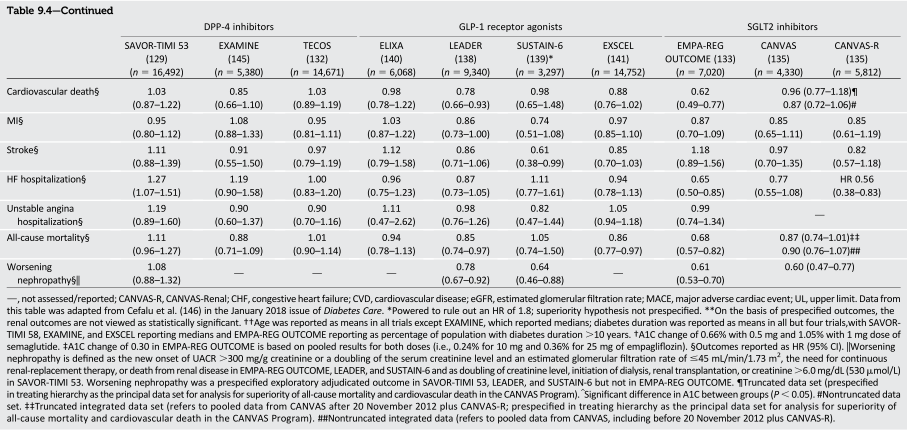
- 加入新的Table 9.4 整合所有CVOT studies

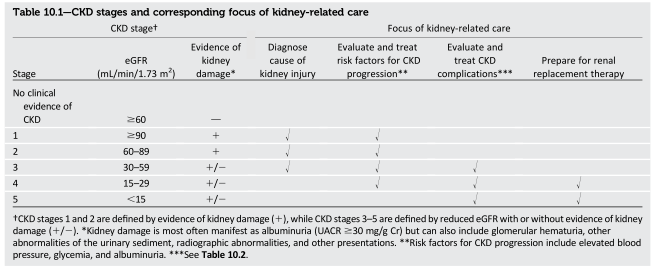
Section 10. Microvascular Complications
and Foot care
- 加入新的Table 10.1 代替之前的10.1
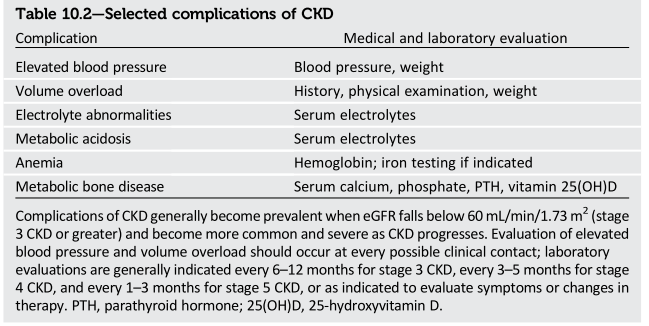
10.2
- 新的Table 10.2 描述CKD併發症和相關醫療與實驗室檢查評估
- 加入關於Acute kidney injury的新章節
- Acute Kidney Injury
- Acute kidney injury
(AKI) is usually diagnosed by a rapid increase in serum Cr,which is also
reflected as a rapid decrease in eGFR, over a relatively short period of
time. People with diabetes are at higher risk of AKI than
those without diabetes (15). Other risk factors for AKI include
preexisting CKD, the use of medications that cause kidney
injury (e.g., nonsteroidal anti-inflammatory drugs), and the use of
medications that alter renal blood flow and intrarenal hemodynamics. In
particular, many antihypertensive medications (e.g., diuretics, ACE
inhibitors, and angiotensin receptor blockers [ARBs]) can reduce
intravascular volume, renal blood flow, and/or glomerular filtration. There
is a concern that sodium – glucose cotransporter 2 (SGLT2) inhibitors
may promote AKI through volume depletion, particularly when
combined with diuretics or other medications that reduce glomerular
filtration. However, existing evidence from clinical trials and
observational studies suggests that SGLT2 inhibitors do not signi ficantly
increase AKI (16,17). Timely identification and treatment of AKI are
important because AKI is associated with increased risks of progressive
CKD and other poor health outcomes (18). (S106-107)
- 討論降血糖藥物對腎病變延遲或加重的影響。
- 加入新建議: anti-VEGF Ranibizumab在有PDR的病人可減少失明風險,和傳統治療(panretinal laser photocoagulation therapy) 相比是non inferiority 。
- 加入新章節,討論高壓氧對糖尿病足的治療。
Section 11. Older adults
- 加入3個新建議, 強調對老年病人個別化藥物治療的重要,在維持A1C目標同時,要減少低血糖風險、避免過度治療以及簡化治療方式。
Section 12. Children and Adolescents
- 加入新建議,治療兒童和青少年的T1D要考慮積極胰島素處方、SMBG、CGM和自動化胰島素傳送系統。
- 加入何時要篩檢celiac
disease 的建議。
- 拿掉了estimating GFR的建議,因為在青少年此公式不準。
- 增加許多關於兒童T2DM的建議。
Section 13. Management of Diabetes in
Pregnancy
- 加入新建議,強調胰島素是懷孕期間控制T1DM和T2DM的優先選擇 。
- 因為有新的證據,加入新建議: 建議T1DM或T2DM的女性在第1孕期末到胎兒出生前 給予低劑量Aspirin (60-150mg/day, usual dose 81mg/day) 來減少子癇前症的風險(建議等級A)。
Preeclampsia and Aspirin
Recommendation
Women with type 1 or type 2 diabetes
should be prescribed low-dose aspirin 60 – 150 mg/day (usual dose 81 mg/day)
from the end of the first trimester until the baby is
born in order to lower the risk of
preeclampsia. A
Diabetes in pregnancy is associated with
an increased risk of preeclampsia (47).
Based upon the results of clinical
trials, the U.S. Preventive Services Task Force
recommends the use of low-dose aspirin
(81 mg/day) as a preventive medication
after 12 weeks of gestation in women
who are at high risk for preeclampsia (48).
A cost-bene fi t analysis has concluded
that this approach would reduce morbidity,
save lives, and lower health care costs
(49). (S140)
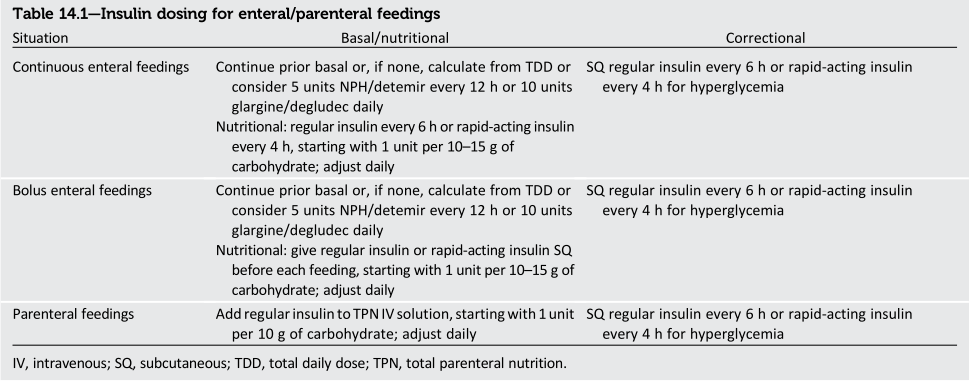
Section 14. Diabetes Care in the
Hospital
- degludec 被加入管灌病人或是Parenteral
feedings的血糖控制選擇中(table 14.1)
沒有留言:
張貼留言